
Recently, first aid and cardiopulmonary resuscitation have become a public topic and have also attracted the attention of ordinary people. Online tutorials and offline first aid training are also on fire.
The 2015 edition of the AHA Guidelines for Cardiopulmonary Resuscitation has also been released for some time, and almost every doctor has seen the interpretation of the guidelines. The comparison between the 2010 guidelines and the 2015 guidelines is the focus of first aid training.
But most of the time, the first aid training teacher is wrong!
What’s wrong?

PPT of Cardiopulmonary Resuscitation Training
Everyone’s statement is very consistent, how can it be wrong? -Because they are copied from each other. If you accidentally pay attention to similar public numbers, you should polish your eyes a little.
First of all, let’s say the conclusion:
In the 2010 guidelines, it is uncertain whether cardiopulmonary resuscitation should be performed for 1.5 to 3 minutes before defibrillation. The new guidelines in 2015 determine that this should not be done.
The correct approach is:
Defibrillation as soon as possible (under no circumstances is it necessary to perform cardiopulmonary resuscitation for 1.5 to 3 minutes before defibrillation), but cardiopulmonary resuscitation should be performed when defibrillators are not ready.
The original English text of the 2010 Guidelines for Cardiopulmonary Resuscitation reads as follows:
There is an incident event to determination if 1 1/2 to 3 minutes of CPR should be provided prior to definition. CPR should be performed while a definition is being read (Class I, LOE B).
There is not sufficient evidence to determine whether cardiopulmonary resuscitation (Class I, Class B evidence) should be performed for 1.5 to 3 minutes before defibrillation when defibrillators are ready.
2015 Guidelines for Cardiopulmonary Resuscitation:
For adults with unmonitored cardiac arrest or for whom an AED is not immediately available, it is reasonable that CPR be initiated while the defibrillator equipment is being recovered and applied and that defibrillator is used as soon as possible (Class IIa, LOE C-LD). For adults with unmonitored cardiac arrest or for whom an AED is not immediately available, if indicated
English is too long to read? Look at AHA’s Chinese version of < < 2015 Summary of Cardiopulmonary Resuscitation Guidelines > >, regarding defibrillation, this is what it says:
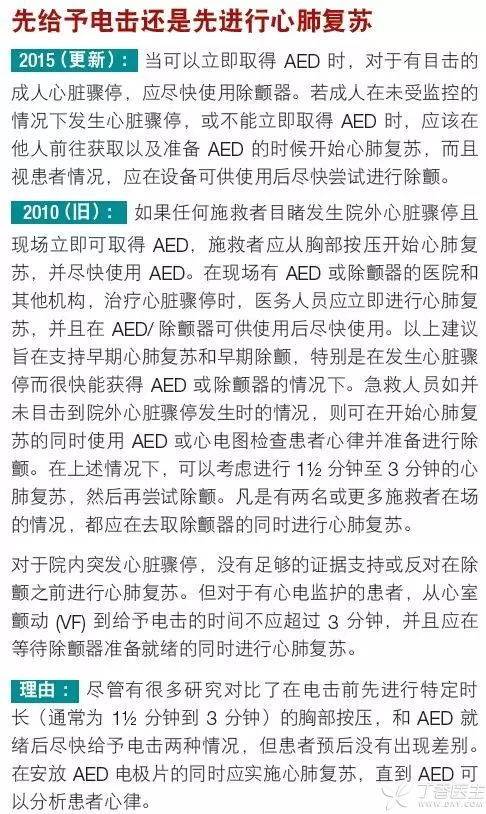
2015 (new): … defibrillation should be attempted as soon as the equipment is available.
2010 (old): Hospitals or other institutions with AED or defibrillator on site, …… Use the AED/defibrillator as soon as it is available……. If the emergency personnel do not witness the occurrence of out-of-hospital cardiac arrest, they can use AED or electrocardiogram to check the patient’s heart rhythm and prepare for defibrillation at the same time as starting cardiopulmonary resuscitation. In the above cases, they can consider performing cardiopulmonary resuscitation for 1 1/2 to 3 minutes and then try defibrillation again.
However, there are two points worth noting in this sentence: first, it limits the situation, only when cardiac arrest outside the hospital is not witnessed; The second is [can be considered], not universal suggestions.
At this point, it can be understood that the previous erroneous statement is actually a misreading of [under the above circumstances, we can consider carrying out…] and has achieved the effect of spreading from one generation to another by [learning from] each other.
It is not enough to read the new guide
Some readers may ask: People are at least right about the contents of the new guide. Just know what to say about the latest guide.
Not so. The 2015 edition of the guide uses a patched writing method, which is:
- If there are updates, write them down and tell you why. Not updated, need to emphasize, emphasize; Do not update, do not need to emphasize, no longer write.
When the 2010 guide was released, it was enough to look at the 2010 guide. Because compared with the earlier 2005 guide, the 2010 guide has subversive changes and is written in particular detail.
Therefore, it is more difficult than before to understand the 2015 guidelines for cardiopulmonary resuscitation-it is not enough to read the 2015 guidelines alone, but to read the 2010 and 2015 guidelines at the same time.
Finally, Clove Garden gives each doctor a little advice and sets an example:
As a doctor, one should have the awareness of evidence-based and textual research, and read the guidelines carefully. When training and guiding others, it is even more necessary to ensure correctness and not to mislead people.