

Neonatal hemolysis, may be a lot of hemp is known from an entertainment news.
Waiting for the upcoming second child is a happy thing, but it is a thrilling process for Treasure Island artist Hou Peicen.
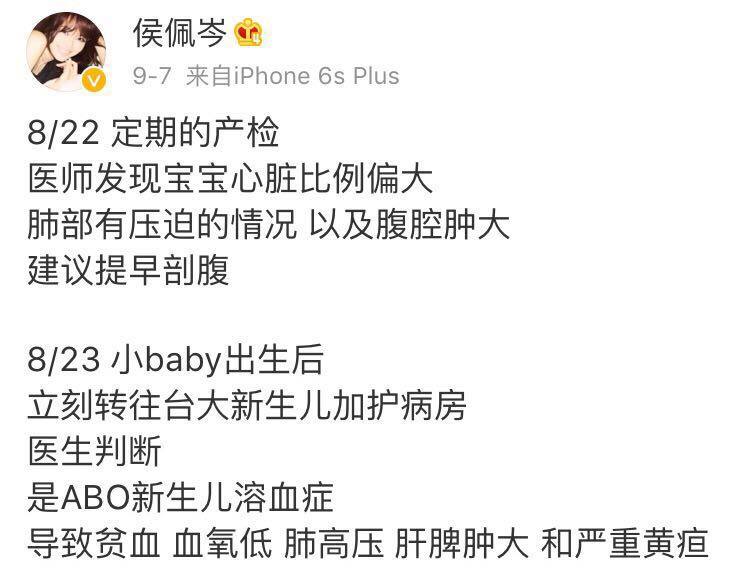
In 2017, Hou Peicen was pregnant with a second child in his stomach. During the prenatal examination on August 22, doctors found that the second child had abnormal symptoms. If he did not give birth by caesarean section early, the fetus would be in danger of life! As a expectant mother, Hou Peicen had to make a choice.
After the baby was discharged from hospital smoothly, Hou Peicen described on Weibo the experience of saving the child by Caesarean section in advance.
After seeing Hou Peicen’s second child suffer from [ABO neonatal hemolysis], netizens also revealed that their child had also been hospitalized for [hemolysis], expressing that they were fully aware of the worries and sufferings.
So is what the [neonatal hemolysis] that worries mothers so much? Mother Clove invited Dr. Wu Feifei to popularize science for everyone today.
After seeing the content of this microblog, Dr. Wu analyzed and said that [ABO neonatal hemolysis] does have a certain incidence rate, but it has little to do with the early caesarean section of Hou Peicen’s baby. The early caesarean section is still due to the problems of large heart and lung compression of the fetus.
What is neonatal hemolysis?
Hemolytic disease of newborn refers to a kind of hemolysis of fetus or newborn caused by different blood types of mother and fetus.
There are many different types of human blood types. Neonatal hemolysis includes many types of hemolysis. The most common one is ABO hemolysis.
To give a simple example, if a mother is of type O blood, the child’s father is of type A blood, and the baby happens to follow the father, and the blood type is not type O, there may be mother-infant blood type incompatibility.
Type O blood mothers are more likely to give birth to babies suffering from hemolysis?
In principle, this is indeed the case:
Because the blood of mothers with type O blood contains both anti-A antibody and anti-B antibody, the probability of incompatibility with the baby’s blood type will be greater.
However, mothers with type O blood need not worry about their husbands’ blood type. Since human reproduction, about 15% of mothers and infants have ABO blood type incompatibility, of which only 4% have hemolytic disease.
Even if ABO hemolysis occurs, most of the symptoms are not serious, such as jaundice in newborns.
Does hemolysis need prevention?

There is only one situation that needs to be prevented, that is, the mother is panda blood (Rh negative blood type).
Mothers of this blood type can be prevented by antibodies when they are not sensitized before delivery.
For other hemolysis cases, as mentioned earlier, the incidence rate of hemolysis is very small, and the symptoms are not serious, so prevention is not of great significance.
Therefore, if mothers are only because of type O blood, then there is no need to worry about the consequences of ABO hemolysis on their babies, so don’t worry about getting pregnant!
How should hemolysis be treated?

Prenatal treatment
The general hemolysis does not need prenatal treatment, except for the mother of panda blood. The mother of panda blood detected abnormal antibody titer during pregnancy and will take measures according to the baby’s situation:
- When the fetal lung is mature, early delivery may be considered. When the fetal lung is immature, intrauterine blood transfusion can be adopted to improve the anemia of the fetus.
Neonatal treatment
If hemolysis is found after the baby is born, possible nervous system damage can be reduced by reducing bilirubin level in blood. Common therapies include:
- Light therapy, Light therapy for short, Simple and effective, When the light shines, it will cover your eyes. Generally, continuous or intermittent irradiation can obtain satisfactory curative effect for 24-48 hours. Drug therapy includes liver enzyme inducer, albumin supplement (plasma transfusion), intravenous immunoglobulin, etc. Exchange blood therapy is required for most Rh hemolytic diseases and some serious ABO hemolytic diseases. Other symptomatic treatments include prevention of hypoglycemia, correction of hypoxia and anemia, etc.