

Hearing loss is the most common congenital birth defect in the world. The incidence rate of permanent hearing loss accounts for about 20% of all birth defects, with the incidence rate ranging from 1/1000 to 3/1000.
Normal listening is a prerequisite for people to learn a language, The brain needs both ears to receive external stimuli continuously before it can acquire language. If children with hearing impairment are not diagnosed and treated in time, they will lose the ability to socialize and learn, bring them difficulties in life and psychological trauma, and eventually become a burden on their families and society.
Hearing impairment in infancy can cause devastating damage to language learning, causing children to be deaf and dumb.
If you can find hearing impairment as early as possible, you can help children learn language through hearing aids, cochlear implants and other treatment methods. China’s newborn hearing screening is a part of the national neonatal disease screening, mainly in order to find children with hearing loss as soon as possible.
How to do hearing screening?
Hearing screening is conducted according to the mechanism by which people obtain sound.
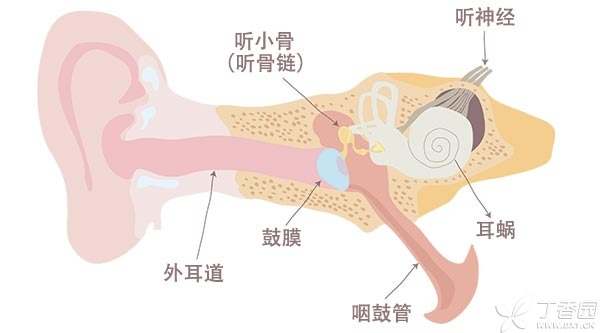
The main process for us to acquire and understand sound is:
-
Sound stimulation is transmitted from the external auditory canal, through the tympanic membrane to the ossicular chain, and then to the cochlea of the inner ear.
-
The cochlea converts the stimulation of sound waves into nerve signals, which are transmitted to the brain by the auditory nerve. Under the integration of a series of neurons in the auditory center of the brain, people hear the sound and understand its meaning.
Hearing screening mainly includes two screening methods: otoacoustic emission and auditory brainstem evoked potential.
1. Otoacoustic emission
It refers to the phenomenon that the normal cochlea will make a sound after receiving external sound stimulation, and this sound will be conducted to the external auditory canal through the ossicular chain and periosteum.
This spontaneous sound can be recorded by instruments, So as to evaluate the function of the cochlea. Because the instrument needs to record tiny sounds, otoacoustic emission examination will be affected by environmental sound, the state of the external auditory canal and the degree of cooperation of the subject. For infants, this examination is more accurate during quiet sleep and can avoid interference with the experimental results such as crying and swallowing.
It should be noted that otoacoustic emission can only evaluate the function of cochlea, not auditory nerve. However, due to the simple operation and wide popularity of the experiment, the first hearing screening is mostly for this item.
2. Examination of auditory brainstem evoked potential
The instrument is used to give the child sound stimulation, and then the bioelectrical activity of the child’s auditory nerve activity is recorded through the electrode piece attached to the child’s head skin, so as to evaluate the function of the auditory nerve and brainstem auditory nerve nucleus.
This examination is also better performed when the child falls asleep quietly. The examination will not be disturbed by the condition of the external auditory canal and is one of the routine items for diagnosing hearing impairment.
The defect of auditory brainstem evoked potential is that it can reflect the disturbance of high-frequency hearing threshold, but it is easy to miss the disturbance of low-frequency hearing threshold.
Summary: Otoacoustic emission can well screen the defects of low-frequency hearing threshold, so the combination of otoacoustic emission and auditory brainstem evoked potential for neonatal hearing screening can fully grasp the hearing situation of children.
Hearing screening in what?
The first neonatal hearing screening is conducted in maternity ward or neonatal ward.
- Normal newborns: Hearing screening is usually carried out from 48 hours after birth to before discharge. If the first screening fails or is not carried out, Re-screening is required 42 days after birth. For children who have not passed the re-screening: Need to be referred to the hearing impairment diagnosis and treatment institution stipulated by the provincial health administrative department for further diagnosis at 3 months after birth. Children hospitalized in the neonatal ward for treatment shall receive hearing screening at the time of discharge. If they fail, they shall be referred to the hearing impairment diagnosis and treatment institution for further diagnosis and treatment.
How do you view the results of hearing screening?
As parents of newborns, they need to remember to check the hearing screening results form issued by the doctor when they are discharged from hospital, which will write the screening results and the time and place of review, and review in time according to the doctor’s advice.
1. False positives may appear in the initial screening.
If the test method used in the initial screening is otoacoustic emission, false positive results may be caused by blockage of amniotic fluid, fetal fat and other residues in the ear canal of newborns, environmental sound interference, middle ear lesions, etc.
Failure to pass the first screening does not necessarily mean that there is hearing impairment, which needs to be confirmed by re-screening. If the reexamination still fails, further diagnosis and treatment should be carried out at the hearing impairment diagnosis and treatment institution.
2. Pass the preliminary screening but have high risk factors,
If the initial screening is passed, but the child has high-risk factors, hearing screening should be conducted once a year for three years after birth. Some hearing impairments will not appear until after the newborn period and need regular testing.
High risk factors include:
- Hospitalization in neonatal intensive care unit (NICU) for more than 5 days; A member of the family with hearing impairment; Diagnosed as intrauterine infection caused by cytomegalovirus, rubella virus, herpes virus, syphilis or toxoplasmosis (toxoplasmosis) disease, etc.; Craniofacial deformities, including auricle and auditory canal deformities, etc.; Birth weight less than 1500 grams; Children suffering from neonatal hyperbilirubinemia and meeting the requirements of exchange blood; Newborns who have been diagnosed with viral or bacterial meningitis; Neonatal asphyxia at birth; Children who have suffered from premature respiratory distress syndrome; Children who have been ventilated for more than 48 hours; The mother used ototoxic drugs or loop diuretics during pregnancy, or abused drugs and alcohol; Clinically present or suspected syndromes or hereditary diseases related to hearing impairment.
3. Attention should also be paid to observation through screening.
Some children with permanent hearing impairment cannot find the corresponding high-risk factors, so even if they pass the hearing screening, parents should pay attention to their children’s response to sound in later life.

Pay attention to observation, find and treat as soon as possible.
Early detection of symptoms of hearing impairment is very important for treatment. Parents can observe their children’s responses to sounds and human voices.
It should be noted that children with hearing impairment can also perceive the world through vision, so parents should not regard the baby’s response to what he sees as what he hears.
Parents can be in a quiet room, let the child lie flat on the bed, in a sober and happy state. At this time, parents can take a bell or other sound toys, shake in the place where the baby cannot see, the baby with normal hearing will turn his head to the sound part to look for. Can change the left and right sides to try.
If you feel that your baby is slow to respond to sounds or cannot start speaking for a long time, Early intervention for hearing impairment should be started within 6 months after birth, through hearing aids, cochlear implants, vibrating sound bridges and other means to help children hear sounds, and then through professional language rehabilitation training to achieve the purpose of deafness but not dumb.
Editor: Yidan