
Taste Map of Tongue
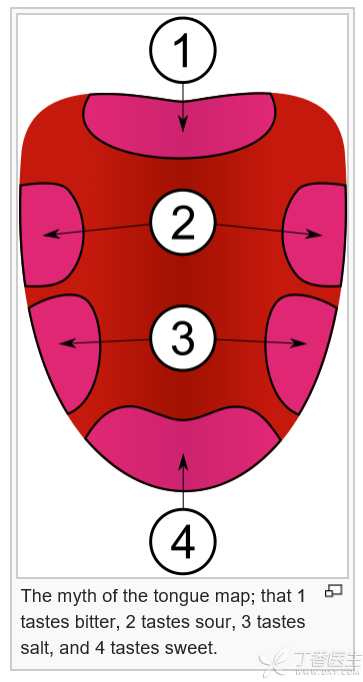
The story of taste distribution map on the tongue [LDC1] (as shown in the figure) is too widely circulated. Everyone has heard that different areas of the tongue are responsible for sensing different tastes. Sour, sweet, bitter and salty are treated separately. According to the map, it seems that only by tasting dessert delicacies with the tip of the tongue can one appreciate their real delicious taste.
This map of the taste buds of the tongue was first proposed by a German, He published a related paper in 1901, Perhaps because this conclusion is interesting and easy to understand, it has been continuously used and passed down to this day. Until 2006, an article on Nature overturned this long-standing statement. The real fact is that the tongue has no taste perception position at all in the Chu-Han River boundary, and taste buds that sense each kind of taste are randomly distributed on the surface of the tongue body.
In addition, in addition to the taste sensations of sour, sweet, bitter and salty, we can actually sense the [fresh] taste. This experience mainly comes from meat, fungi or monosodium glutamate, and most of the cases are related to free amino acids in food.
If you tear up rumors, you must have good evidence.
In some non-serious medical media or mass media, it is often seen that some types of reports are [so-and-so well-known experts say that what medicine is easy to use and how to treat what]. Regardless of the true or false identity of [experts], judging whether a medical knowledge is reliable does not depend on experts, but on evidence. One cannot believe all the words of one family.
Evidence-based medicine (EBM) means “evidence-based medicine”. Its central idea is that medical decisions (i.e. Patient treatment, treatment plan, etc.) should be made on the basis of the best clinical research.
The same [evidence] is also good and bad. Therefore, WHO proposed GRADE evidence quality classification system.
The best evidence often comes from randomized controlled studies (RCT), while other observational studies, expert opinions and case reports are less credible.
If this is the case, the level of evidence will be reduced: the quality of the test is not good; The research results are inconsistent. It is not certain whether it is direct evidence; Inaccurate data or too few samples; There is a great bias.
Correspondingly, studies with these characteristics have a higher level of evidence: the effect value is large, and there may be confounding factors affecting the curative effect; There is a clear dose-response relationship.
If doctors do not have the energy to analyze the evidence strength of each document, what should they do?
Multicenter randomized controlled studies, or a combination of a series of strong evidences (e.g. Meta-analysis and systematic review combining multiple RCTs), have relatively consistent results, which are often highly convincing.
Some special tests (especially in the food and drug industry) will also be supported by funds from companies and enterprises with direct interests, so they cannot be trusted.
A more convenient method is that mature research can refer to the latest international guidelines, which are often the conclusions drawn by experts according to a large number of studies, and can be used as a reference. In addition, you can consult evidence-based medicine websites or databases such as Cochrane Library, uptodate, DynaMed, etc.
For new research, we should try our best to refer to authoritative journals, such as Nature, Science, Cell and Medicine.