In the semi-finals of the women’s badminton singles at the Rio Olympics, China’s Li Xuerui accidentally sprained his leg during the fierce confrontation with the Spanish player and was later confirmed to have completely broken the anterior cruciate ligament, regretfully ending his trip to the Olympics.
Anterior cruciate ligament is a common sports injury of knee joint, which usually occurs in the following situations:
- Suddenly change the direction of movement, slow down during running, jump off the knee joint and touch the ground, such as sprain in football.
If this ligament is completely broken, it may easily sprain the knee repeatedly in later life, and the patient often feels unstable when walking and running. Therefore, after sprain, the patient dare not accelerate to do fast running, sudden stop and sharp turn, and cannot complete single-foot landing and shooting, which seriously affects daily life and generally requires surgical treatment.
However, after ligament repair by surgery, rehabilitation treatment is a more critical part and cannot be ignored. Its therapeutic effect will directly affect the future mobility of the knee joint.
Therefore, rehabilitation training should be carried out in a planned way under the guidance of professionals. Rehabilitation training is mainly divided into knee joint mobility training and muscle training.
First, knee joint mobility training
If the knee joint is not moved after the operation, the soft tissue of the knee will gradually adhere, and finally the joint will become stiff and the knee joint cannot be straightened and bent normally.
Therefore, the knee joint should be moved as soon as possible after the operation, and straightening and bending training should be done. Pain is inevitable when the joint is moved early after the operation. Patients should relax as much as possible. Fear and nervousness will aggravate the pain and affect the activity effect.
Activity training mainly includes straightening and flexion exercises:
Step 1 Exercise straightening
Remove the brace, raise the affected limb and put it on the pillow with the toes facing directly above and the knees empty, so as to ensure that the knees are straightened (Fig. 1) for 15-20 minutes each time and 3 times a day.

Step 2: Buckling exercises
Knee pain and swelling are obvious 2 weeks after operation, and passive bending can be done with the help of doctors or physiotherapists (Fig. 2).

After the pain is slightly relieved, the patient can sit on the bed with his lower leg drooping, then put the healthy leg on the affected leg, or tie some sandbags on the affected leg to do some exercises of actively flexing the knee joint (Fig. 3).

Buckling exercises should be carried out step by step, not only to stick to exercises every day, not slack off, also can’t delusion to achieve overnight, excessive practice. Each time to stick to practice for 15 minutes, once a day. At the beginning of the knee joint can only be within the range of 0 ~ 60, after every day to improve 10 ~ 15 than before, generally 2 weeks later the knee joint can actively bend to 90.
After 2 weeks, the knee flexion will not be so painful, and the training methods will be more varied at this time. By frequently doing [supine hanging legs], [clasping knees with both hands] and [prone hooking legs], the knee bending angle will gradually reach normal and finally approach the level of the healthy side.
Supine leg hanging: suitable for 100 ~ 110 flexion range. First lie on your back with your thigh perpendicular to the bed surface, relax your thigh muscles, and add a little weight to the ankle joint to allow your lower leg to droop naturally under the action of gravity and weight bearing, as shown in the figure (Fig. 4).

Hold your knees with both hands: suitable for 110 ~ 130 range of motion, such as (Fig. 5). This method is simple and convenient, and is the most commonly used method.

Prone leg hook: The patient is required to lie prone first, actively bend the knee to the maximum angle, then put an inelastic belt on the ankle to passively increase the joint flexion angle, so that the joint flexion angle can reach 120 ~ 135 degrees, as shown in Fig. 6.

Knee straightening and flexion exercises are arranged in the morning and afternoon respectively, and ice is applied for 15-20 minutes after the end, which is a good way to relax the knee and relieve discomfort symptoms.
Second, muscle training
Rest is the main method in the early stage after operation, and the physical activity that can be done is very limited. Muscle atrophy is easy to occur, which affects the subsequent rehabilitation and the final joint strength and flexibility. Therefore, muscle strength training should be carried out as soon as possible and as much as possible. Muscle training generally does not cause pain, and patients need not be too nervous.
Isometric training of thigh muscles: When the thigh is stretched, the quadriceps femoris on the front side of the thigh contracts, and when the thigh is pressed down hard, the muscles on the back side of the thigh contract, and then relax into a group of exercises. After anesthesia subsides, you can start and do as much as possible.
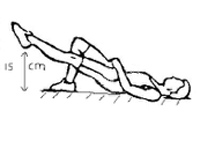
Straight leg lifting: The knee is completely straight, the leg is raised by about 15cm, and the posture is maintained until exhaustion. Each exercise interval is 5 seconds, each group does 10 times, and each group insists on 3-4 groups every day (Fig. 7). If the pain can be tolerated, the operation can start on the same day. If the pain can’t be tolerated, the operation can start 2-3 days after the operation, but not later than 3 days.
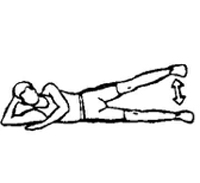
Similar training to straight leg lifts includes side leg lifts (Fig. 8) and rear leg lifts (Fig. 9), both of which keep the knees straight.

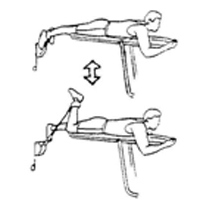
Progressive resistance training of lower limb muscles can be started 2 months after the operation, and the strength of the three main leg muscle groups (quadriceps femoris, hamstring and triceps calf) can be strengthened in a targeted way. Including [resistance knee extension] (Fig. 10), [resistance knee bending] (Fig. 11), [slow squat] (Fig. 12), etc.